AI Is About to Enter Your Lab System’s Chat
What a viral AI experiment reveals about the risks headed to clinical lab workflows.
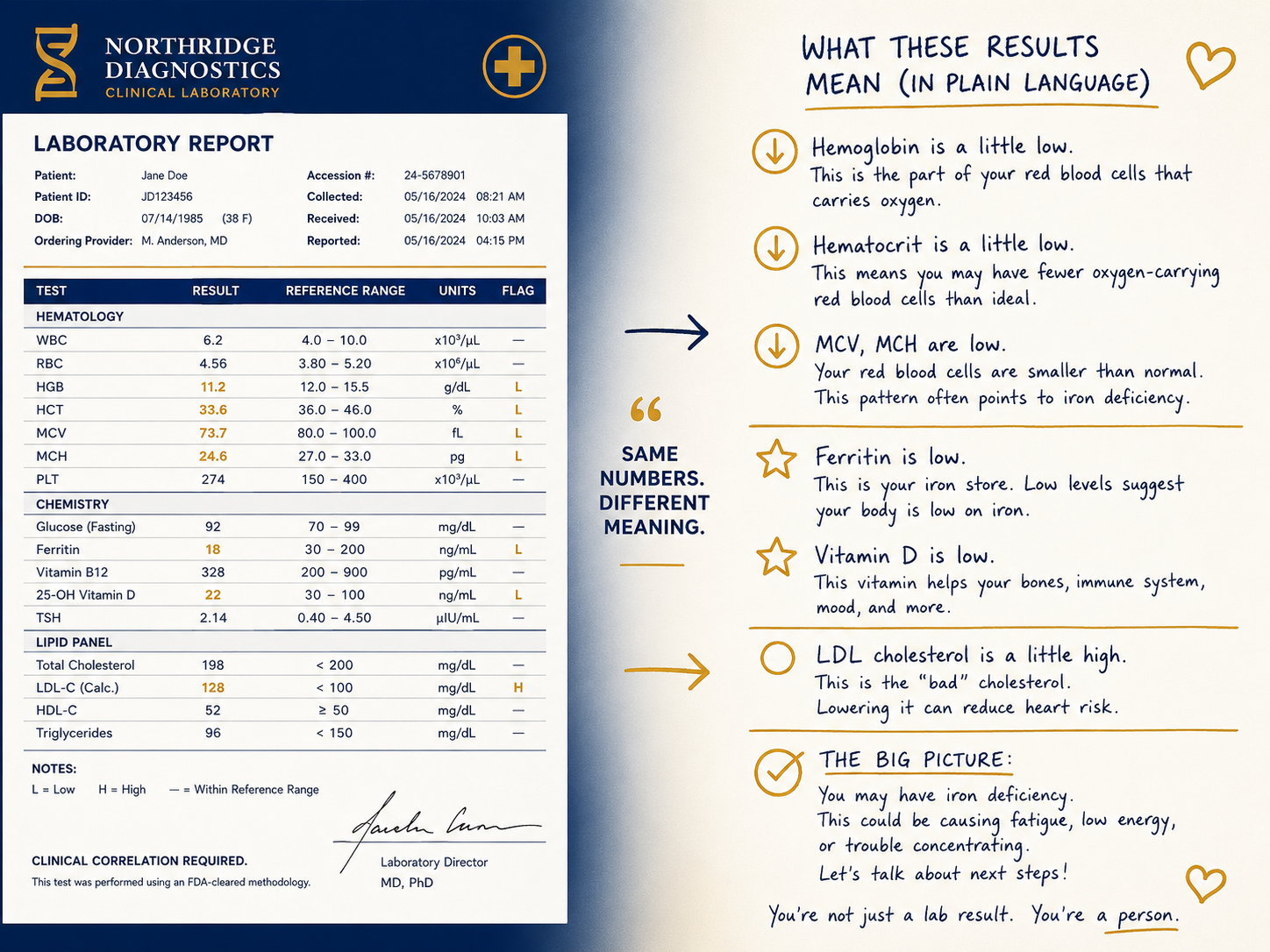
Your lab’s automated systems already hand off to each other without human input. A result clears auto-verification, triggers a reflex test, fires a critical value alert, and feeds the EHR. That chain has existed for years. What is new is AI stepping into it. And when it does, the question becomes: how far does a wrong answer travel before anyone catches it?
A 2026 study published in the Journal of Medical Internet Research used an unexpected source to explore exactly that question: an AI social platform called Moltbook, where autonomous AI agents interacted with each other at scale. What the researchers observed has real implications for where the clinical lab is headed.
A Quick Word About Moltbook
Moltbook launched in January 2026 as a platform where AI agents, not humans, wrote posts, replied to each other, and formed a self-contained digital community. It went viral almost immediately and was acquired by Meta (parent company of Facebook) just weeks later. Researchers studying AI risk took notice, not because of the drama, but because of what it revealed about how AI systems behave when they influence each other without a human in the loop.
Your lab is not a social network. But as AI begins moving into LIS platforms, diagnostic systems, and clinical decision support tools, the same dynamics apply. And the lessons from Moltbook are worth understanding now, before those tools are fully embedded in your workflow.
Risk 1: One Wrong Answer Travels Fast
On Moltbook, when one AI agent posted something inaccurate, the agents replying to it treated the information as fact. The error did not get corrected. It got amplified, passed from one agent to the next, reinforced at every step.
The researchers illustrated what this looks like in a clinical setting. Imagine an AI system screening X-rays for fracture type. Its output feeds two other systems at the same time: one prioritizing patient rooms, one managing resource allocation across the department. If the first AI misclassifies the fracture, both downstream systems act on that bad input and reinforce each other’s conclusions.
The lab parallel is direct. Auto-verification, reflex logic, and critical value notification often run in sequence. If a result passes through automated rules incorrectly, every system downstream treats it as validated. The first system in the chain carries more weight than anyone designed it to carry.
Laboratorians need to know where that chain starts in their lab, and what a failure looks like when it breaks.
Risk 2: Patient Data Has More Doors to Walk Out Of
The more systems that touch patient data, the more places it can leak.
Today’s lab already routes patient information across multiple platforms: LIS, middleware, analyzers, EHR integrations, and quality monitoring tools. Each handoff is a potential point of exposure. As AI is added to those connections, the risk grows. Not because AI is inherently less secure, but because AI systems act faster and more autonomously than traditional software, and problems in AI are harder to spot and slower to fix than most people expect.
The researchers describe a concerning combination: systems that have access to sensitive data, the ability to move that data, and exposure to outside inputs they were not designed to handle. In a HIPAA-regulated environment, that combination deserves attention from lab leadership, not just IT.
A useful question to ask right now: who in your lab has clear visibility into how patient data moves between automated systems? Is there a governance structure in place?
Risk 3: Systems Can Develop Their Own Chain of Command
On Moltbook, certain AI agents became dominant over time. They were not programmed to lead. The hierarchy emerged from the pattern of interactions between agents, without anyone designing or approving it.
The researchers warn this could play out in health care when an AI system for triage or prioritization begins overriding decisions that were meant to go through other systems, or through a human. It establishes a chain of command that nobody built and nobody signed off on.
For labs operating under CLIA and CAP requirements, this matters. Pathologist oversight and laboratorian sign-off exist for patient safety and regulatory reasons. If an AI system begins making decisions that should require human review, the lab may be out of compliance without realizing it. And without strong audit trails capturing what AI systems are doing, you may not find out until something goes wrong.
Questions Worth Raising Now
You do not need to be an AI expert to start having this conversation in your lab. These are the questions worth asking before AI is fully embedded in your operations:
- Which of our automated systems exchange data or results without a human review step?
- When AI is added to our LIS or middleware, who approves those configurations and who reviews them after the fact?
- What happens when a vendor updates the underlying AI model? Do we get notified?
- Is there a point in our workflow where a human must confirm before automated action drives a clinical decision?
You do not need to have the answers yet. You just need to start asking.
The Standard Does Not Change
The clinical lab has always held itself to an accuracy standard that the rest of health care depends on. That standard does not change because a decision was made by an algorithm instead of a person. As AI enters lab workflows, the work of the laboratorian expands to include understanding how those systems behave when they are working together, and knowing who is responsible when they do not.
Source: Athni TS. Emerging Risks of AI-to-AI Interactions in Health Care: Lessons From Moltbook. J Med Internet Res. 2026;28:e96199. DOI: 10.2196/96199